

Losing Faith

“Primum non nocere. First, do no harm.” –Hippocrates
I awoke with a start, sweating. There was a pit in my stomach and my body was overheating. My chest felt tight and heart was racing. I groped for my cell phone to check the time. Two o’clock in the morning for God’s sake.
Just like yesterday, I thought. When will I sleep through the night, I asked myself despite knowing the answer. Never. Frustrated with myself, I got up and put on a robe to make my way to the kitchen.
Making tea gave me a few minutes reprieve when I didn’t need to think of anything at all. All my thoughts were put on hold from the moment that I put the tea kettle on the stove until the satisfying wafts of bergamot and vanilla a few minutes later. With the first sip, I had to face reality again.
The problem was that my faith in his oncology team had grown thin, which amplified my fears for his health. On the day he nearly died, he woke up in good spirits. But by mid-afternoon, he nearly collapsed after only mild exercise on the tennis court. The clot that nearly killed him had likely been there for months and his complaints of arm swelling had been brushed off. His doctors made a big mistake in dismissing his symptoms, and I wasn’t ready to forgive them yet.
Ironically, my anger wasn’t diminished by the knowledge that I had also made mistakes as a physician. Could I call the kettle black if I myself was a small black pot? Yes, I most certainly could. There were BIG differences in the mistake that I had made versus the one that his doctors had made, I reassured myself.
One mistake that I recall centered on a Somali refugee in her early twenties that I treated when I was a young resident physician, not more than 6 months out of medical school. She escaped a brutal civil war and famine only to languish in a Kenyan refugee camp for several years with her mother and siblings. I didn’t know what happened to her father but guessed that he had been killed in the war. Her family was fortunate to be chosen to resettle in the United States. Some people would never leave that Kenyan refugee camp and would live out the rest of their lives there.
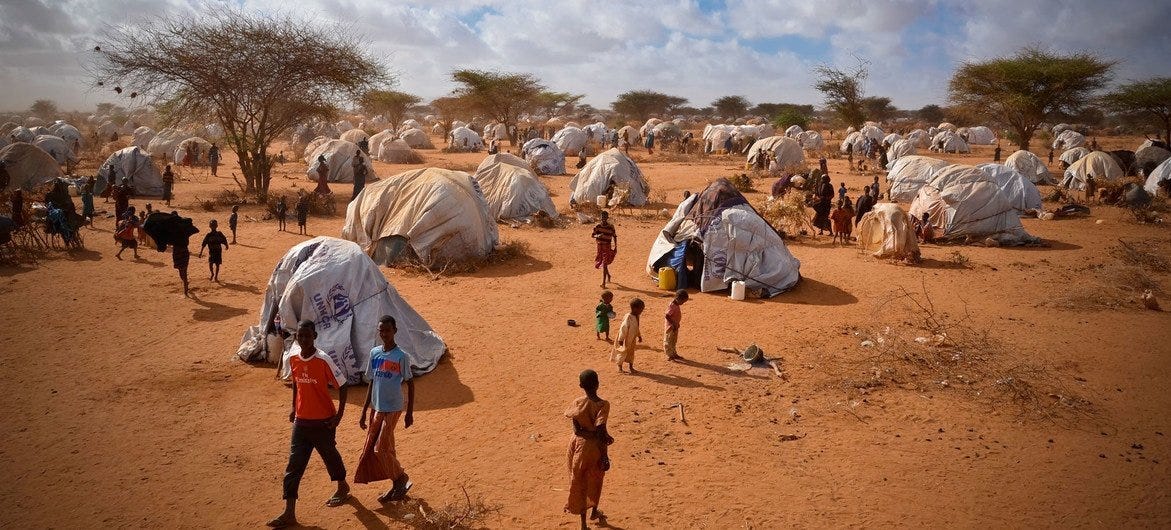
Somali Refugee Camp (Kenya)
Most of my Somali patients kept their trauma very private and focused only on their physical symptoms in our visits. But the psyche and physical body are difficult to disentangle. What she had experienced during her flight from Somalia wasn’t technically part of our visit, but how could one fail to account for the deep trauma that many refugees had experienced. They fled war, walked for weeks without food or much water, endured sexual assault, and witnessed family members being killed. Physical symptoms are often a manifestation of psychological pain, which I recognized in my patients over and over.
The patient was wearing a navy-blue hijab and ankle-length dress leaving only her creamy, brown face and hands exposed. Her eyes were downcast, and she looked up only briefly to make eye contact with me in our first visit. I guessed that she might be depressed and made a note to ask her later about her mental health. Depression, anxiety, and post-traumatic stress disorder were common in refugees. Operating from the assumption that the refugee patient sitting before you had survived unspeakable evils and needed care for their mental health was a good rule of thumb.
“She has back pain,” the female interpreter began as I entered the room. “It started a year ago before she came to the U.S.,” the interpreter continued before I had a chance to launch into my standard list of questions: where the pain was located, how severe was the pain, how long had it been ongoing, did the pain radiate anywhere, and any other symptoms. Our interpreters spent most of their days in our clinic and within a short time could somewhat predict our series of medical questions.
The patient with downcast eyes had lower back pain that was slowly worsening. Beyond this general description, I struggled to get more information, probably due in part to the language barrier and my own inexperience. I couldn’t tell you the first thing about her life in the U.S. or in the camps, or whether she routinely lifted heavy items (like vessels of water). Did her pain start after lifting something heavy? Or in response to a traumatic event? Was she lifting young children at home and balancing them on one hip?
I performed a perfunctory exam, pushed on the muscles in the back and along her spine. She jumped a few times during the exam, but I couldn’t pinpoint any specific location for the pain. Sending her off to physical therapy seemed like a reasonable first step.
My experience evaluating back pain was rudimentary at best and another doctor would probably have handled this case much better. I was a brand-new obstetrician-gynecologist in training and my experience in this area came from a 6-week neurology rotation that I had two years before this visit. I also wasn’t very knowledgeable about the conditions that might be present in refugees or travelers from the Southern hemisphere. More than anything, I hoped that my physical therapy prescription would help, and she wouldn’t need to come back.
But the patient with the downcast eyes kept coming back. She wasn’t any better despite physical therapy and the pain was in fact getting worse. I think it was on her third visit over a 6-month period that my supervising physician came into the room with me to supervise my exam.
I vividly remember her knee reflex on the right side because it took me by surprise. The supervising physician had seen it too and had the same reaction. To convince myself that I wasn’t seeing things, I repeated the maneuver starting on her left side. I gently hit a spot below her kneecap with my reflex hammer. The left leg kicked out in a familiar cadence. Nothing unusual there. The right knee reflex should look just the same.
When I hit the right knee with my reflex hammer, the effect was muted. Her right leg hardly moved, a motion that was less than half as pronounced as on the left side. A decreased patellar tendon reflex may mean that she has spinal cord disease or injury, I thought to myself, and my stomach churned. She needed an X-ray at the bare minimum and likely a referral to neurology.
The X-ray showed classic findings of Pott’s disease, another name for a tuberculosis infection of the spine. One of her vertebrae had collapsed and the shadowing next to the area with whitish calcifications indicated a probable abscess. Tuberculosis is an infectious disease that typically attacks the lungs but can spread through the blood to other places in the body. In the spine, tuberculosis can cause nerve damage, paralysis, and even back deformities. The delay in her diagnosis may have led to more damage in her spine.

[This is an MRI image of Pott’s disease of the spine (spinal tuberculosis) in another patient that I found on Creative Commons. In the middle of the image, note the whitish area in the spinal column indicating an abscess, an infectious fluid collection of tuberculosis bacteria. ]
How I missed a diagnosis like this over three visits, I can’t explain. If I am kind to myself, I imagine that the abscess may not have been there when I first saw her. If I am kind to myself, I invoke the language barrier as the reason that I didn’t pick up on more concerning symptoms. But this wasn’t entirely correct. Our clinic interpreters were excellent, and the neurologic exam spoke for itself. There were plenty of signs that this wasn’t the run-of-the-mill back pain in a twenty-year-old Somali refugee.
In short, my error boiled down to my youth and medical inexperience with a disease that I had only heard of when studying for my medical boards. Had my husband’s oncology physician-in-training been so different? He also had at least two opportunities to diagnose the clot. Maybe this was the first portacath clot that he had seen. How could I forgive myself and not him? Was there no limit to my own hypocrisy?
I also couldn’t help wondering whether a woman with breast cancer and arm pain and swelling would have been taken more seriously. Would his doctors have acted on his symptoms if he didn’t appear so strong and dissimilar from their other frailer female patients? Maybe their guard was down, because he was a 6-foot 6-inch man, who rarely complained and seemed to be flying through the toughest course of chemotherapy drugs. He was an unusual patient in their clinic, they told him time and time again. Perhaps this came with assumptions and biases.
Or perhaps the problem was me. What if I had been more forceful in demanding an evaluation for his arm pain and swelling? I didn’t want to dictate his care as a physician because I honestly didn’t know this field. In the process, I think I had so muted my own voice that I failed him as an advocate.
Regardless, the health care system that was supposed to keep him safe had failed. I put my mug on the counter and made the decision to return to bed. I would lay down and hope that in the dark I might fall asleep.
Just before closing my eyes, I remember thinking that we should get a second opinion at a different oncology center.
Don’t delete anything please. I was not offended. This is an unbelievably difficult process. My deepest respect for anyone who has gone through it.
Very powerful and well written. Your writing pulled me in left me wanting to read more, no matter how sad the story. Keep up the great writing!