

100 Different Fonts
After He Said Cancer | A Memoir

There were five of us around the breakfast table of this small bed and breakfast, talking and conversing about medical and scientific topics. We had been perfect strangers the night before but fell into a deep conversation over a glass of wine about the science behind the COVID-19 vaccines. One gentleman and his wife were particularly inquisitive with matching sets of fiery blue eyes.
“So, why isn’t there a treatment for breast cancer?” he asked. “It seems that they have spent a lot of money on it and part of me wonders whether there is an incentive for the drug companies to not find a cure.”
I understood where his question was coming from. He was an entrepreneur, who was still running a successful business in his early 70’s. There was no reason to expect that he would also be well versed in molecular biology and the difficulties with finding a ‘cure’ for cancer. Our professional careers were light years apart. Likewise, I couldn’t understand a company’s balance sheet despite my husband’s patient explanations. But show me data from a scientific experiment and I could hardly contain my enthusiasm to figure out what was going on.
“Great question,” I said, as a metaphor began to take shape in my mind. “Imagine that I print out the word ‘CANCER’ on a piece of paper. Now imagine that I print that same word but use 100 different fonts. Then, I take those 100 different fonts and start randomly capitalizing words and throw in a few misspellings. Next, I replace some of the letters with different colors every now and again. The result is the same ‘word’, but in a thousand different variations. That’s cancer, in a nutshell.”

“Ok. So, what you’re saying is that there are so many variations of cancer that it is impossible to come up with a cure,” he said.
“Not exactly. It’s just challenging,” I sighed. “Even within the same individual, cancer cells may differ quite a bit from one another with different fonts and misspellings. Now, imagine you give a drug to kill a billion cancer cells making up a small tumor. Perhaps 99% of those cells die but there is something peculiar about 1% of the cells. They don’t die and instead become stronger and start dividing. These cells were resistant to that first treatment. To kill off these remaining cells, you likely need a second treatment of some kind.”
“Another possibility,” I continued, “is that 5% of the cancer cells are not dividing very quickly and lying dormant in a place where it is hard for cancer drugs to reach. Many cancer drugs target the quickly dividing cells, but they have trouble attacking the sleepy cells.”
I took a bite of my oatmeal. I thought of the sleepy little cancer cells that often hide in the bone marrow and can awaken after many years of a patient being in remission. They can start to circulate in the bloodstream and cause a metastasis, or simply show up as a metastasis to the bone. I worried a lot that my husband might already have cancer cells in his bone marrow. Just waiting and biding their time.
“Ideally, a cancer treatment would take cancerous cells from the patient and engineer the person’s white blood cells to attack and destroy those cancer cells,” I said, pouring myself another cup of tea. “It sounds like science fiction, but it’s not. It just isn’t a treatment that is ready to adapt to all kinds of cancers or to many people.” I started to wonder if this group would press me to explain how this worked, which was pushing the boundaries of my knowledge.
Digging far back in my brain, I could tell them that CAR T-cell therapies engineered one’s white blood cells (T-cells) to attack one’s own cancer cells. In the therapy, they would collect a person’s T cells and engineer them in the laboratory to attack the cancer cell. It was mainly used for treating blood cell cancers like lymphomas and leukemias that were very different from other cells in the body. There was a lot of interest in adapting CAR T-cell therapies to other cancers.
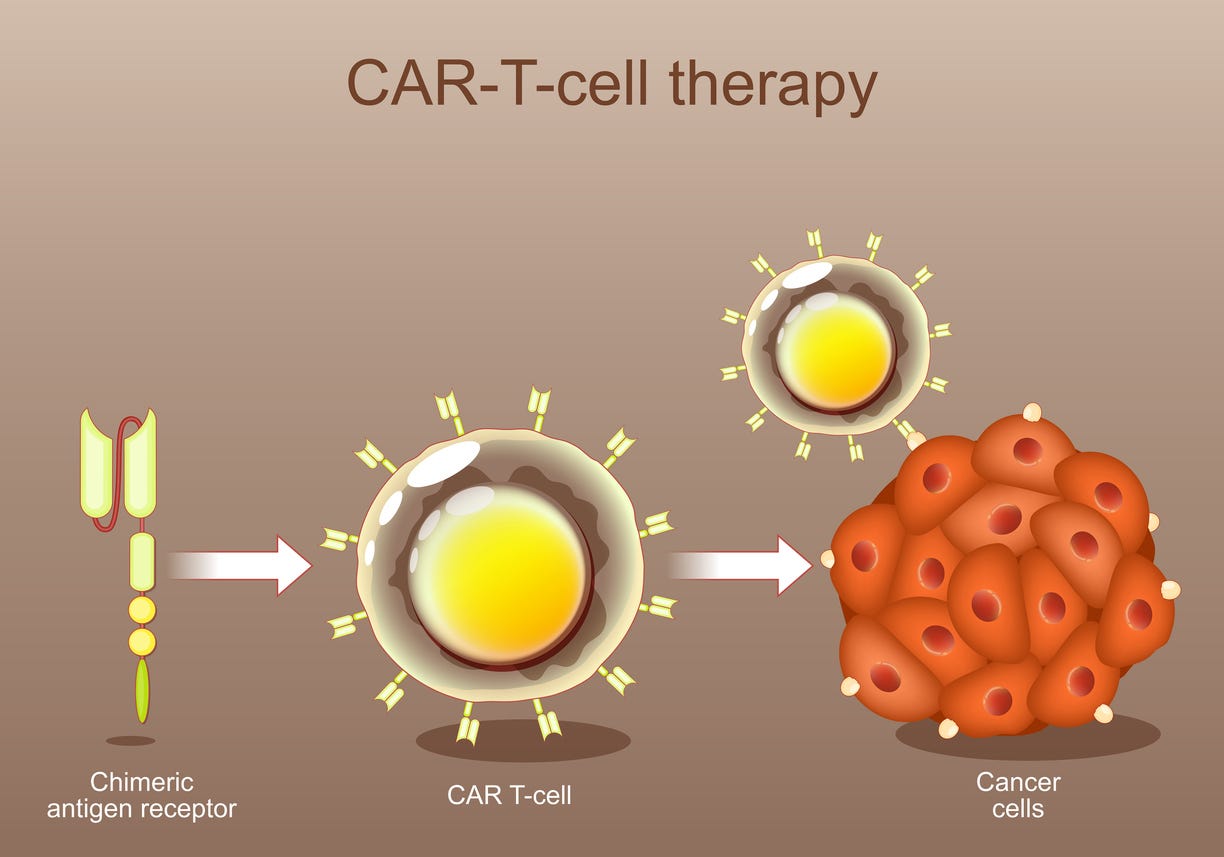
If I got cancer, I would want a CAR T-cell therapy as fast as I could possibly get it. The idea of my T cells wearing Ninja suits, sneaking around my body, on a seek and destroy mission to kill cancer cells was amusing. Personalized medicine at its best.
“Thank you, doctor,” the gentleman said with a respectful use of my title. “Can they use that kind of strategy for breast cancer?”
“Another good question,” I said. I was aware of an effort to apply CAR-T therapy to a specific type of breast cancer with the highest mortality, which didn’t seem to express the usual hormone markers. Fortunately, men didn’t seem to get this type of breast cancer.
“I have a lot of hope that a personalized approach to cancer that harnesses one’s immune system will be developed for many types of breast cancer,” I said. “The science isn’t there yet, but every decade there are big changes in cancer care that make me hopeful for what’s around the corner.”
The man posed another excellent question to the other couple, and I was off the hook for the moment. I looked down at my plate. I had been so busy answering questions that I had hardly touched my food, and I was hungry. A basket of scones caught my eye.
Cancer treatment was a high-stakes game. If you kept trying different treatments and prolonging your survival, maybe an even better cancer treatment would become available. Even in the short time that we had known about my husband’s breast cancer, a new drug called Verzenio was being recommended for patients at high-risk. This drug was the first in a very long time to prolong survival.
“How long until this immune therapy to fight cancer might be available to me?” said the man. He had disclosed the prior evening that he had been treated for prostate cancer.
“If we are talking about men’s health, I must confess that I am out of my comfort zone,” I said, spreading jam on my scone. “But I think drug companies actually have a BIG incentive to make personalized cancer therapies available for all cancers, including prostate cancer. Their incentive to make money hinges on their ability to make a blockbuster cancer treatment, which is exactly what we are hoping for too.”
Maybe, when my husband needed a CAR-T therapy, it would be ready.
*****************************************************************
If you would like to read other posts, here are a few:
How It Began. This story is the origins of my Substack and tells the story of the first moment when we learned of my husband’s breast cancer diagnosis. https://www.afterhesaidcancer.com/p/how-it-began
Dandelions in the Lawn. https://open.substack.com/pub/tigerinmykitchen/p/dandelions-in-the-lawn?r=1acedj&utm_campaign=post&utm_medium=web&showWelcomeOnShare=true
The Day He Proposed. https://www.afterhesaidcancer.com/p/along-the-salish-sea?r=1acedj
Surrender. https://www.afterhesaidcancer.com/p/surrender?r=1acedj
*****************************************************************
Thank you for being one of my readers. I appreciate you very much! If you’d like to support my work you can do so by:
Hearting this post, so that others are encouraged to read it
Leaving a comment (I do my best to respond to each of them), which increases engagement and visibility of my posts
Sharing this post by email or on social media
Taking out a free or paid subscription to this Substack
Leaving me a tip by buying me a coffee.
Thank you so much for this. A great explanation for what science is up against. I wish I could get anyone who has personal experience with cancer to read this.